The significance of minimal residual axillary disease, specifically micrometastases, following neoadjuvant systemic therapy (NST) remains largely unexplored. Our study aimed to elucidate the prognostic implications of micrometastases in axillary and sentinel lymph nodes following NST.
This retrospective study analyzed primary breast cancer patients who underwent surgery after NST from September 2006 through February 2018. All patients received axillary lymph node dissection (ALND), either with or without sentinel lymph node biopsy. Recurrence-free survival (RFS)-associated variables were identified using a multivariate Cox proportional hazard model.
SLNmi is a negative prognostic factor significantly associated with additional non-SLN metastases, while ypN1mi does not influence the prognosis compared to ypN0. Hence, additional ALND may be warranted to confirm axillary nodal status in patients with SLNmi.
The prognostic importance of axillary lymph node (LN) metastases in breast cancer has been well established [1]. Traditionally, axillary lymph node dissection (ALND) served as the standard surgical treatment of invasive breast cancer until the 1990s [2]. Since then, sentinel lymph node biopsy (SLNB) has emerged as a viable alternative, offering an accurate prediction of axillary nodal status while mitigating the higher morbidity rates associated with ALND [3, 4].
In the neoadjuvant context, patients with clinically lymph node-positive (cN+) status underwent ALND, independent of their neoadjuvant systemic therapy (NST) response [10]. However, recent trends advocate the judicious avoidance of ALND in patients who transition to clinically lymph node-negative (cN0) status post-systemic therapy, especially in the absence of metastases in a sufficient number (≥ 3) of sentinel lymph node (SLN)s [11,12,13].
Previous research on minimal residual axillary disease, particularly oncologic outcomes of patients with ypN1mi, after NST has been limited. Furthermore, the evidence regarding additional metastasis in patients with SLNmi is not clear, and consequently, ALND persists as the standard treatment for these patients [14]. This study aims to investigate the significance of pathologic lymph node-micrometastases (ypN1mi) following NST, in comparison to pathologic lymph node-negative (ypN0) or macrometastases (ypN+). We further explore the prognostic implications of SLNmi for the prediction of axillary LN status and survival outcomes.
We conducted a retrospective review of primary breast cancer patients from the registries of Gangnam Severance Hospital and Severance Hospital, who underwent surgery following NST between September 2006 and February 2018. The regimen for NST consisted solely of chemotherapy for HER2-negative patients, while both chemotherapy and anti-HER2 therapy were administered to HER2-positive patients. In our cohort, no patients received neoadjuvant endocrine therapy. These patients were clinically diagnosed with stage II or III breast cancer and underwent ALND, with or without SLNB. Exclusion criteria comprised of patients who had upfront surgery, underwent only SLNB, or presented with de novo stage IV disease.
Our study adhered to Good Clinical Practice guidelines and the principles of the Declaration of Helsinki. The institutional review boards (IRB) granted study protocol approval (approval number: 3-2023-0214). The retrospective study design warranted a waiver for the requirement of written informed consent by the IRB.
The initial axillary nodal status was evaluated using physical examination, ultrasonography and breast magnetic resonance imaging (MRI). Fine needle aspiration biopsy (FNAB) was conducted on patients where necessary. We classified clinical nodal status based on the clinical staging of the anatomic stage system in the American Joint Commission in Cancer (AJCC) 8th edition, with reference to the results from imaging modalities and FNAB [15]. cN0 was defined as the absence of LN metastases on imaging and physical examination, and cN + was defined as the presence of LN metastases in either imaging or physical examination. Patients with metastatic LN revealed by FNAB were categorized as cN+. Furthermore, we classified suspicious LNs on imaging modalities as cN0 if they yielded negative results on FNAB.
Pathologic nodal status was also evaluated based on the pathologic stage of AJCC 8th edition’s anatomic staging system [15]. We defined metastatic LNs with a size range between > 0.2 mm and ≤ 2 mm as ypN1mi, regardless of the metastatic LN count. LNs exceeding 2 mm were classified as ypN+, and ypN stage was assigned based on the number of LNs, inclusive of micrometastases. Moreover, isolated tumor cells measuring ≤ 0.2 mm were classified as ypN0.
SLNB was performed using single or dual tracers. For the single tracer technique, Technetium 99, a radioactive substance, was administered periareolarly prior to surgery, and SLNs were identified intraoperatively via a gamma detection system (Neoprobe ® ). The dual tracer method employed both an isosulfan blue dye and Technetium 99 concurrently. The choice of SLNB technique was contingent upon the surgeon’s discretion. SLNs were categorized as one or multiple, and any LN identified by either or both methods was defined as SLN. LNs resected during SLNB without tracer signal were not classified as SLNs.
ALND was characterized by the removal of all LNs in axillary levels I and II. Patients documented to have undergone ALND in surgical records were primarily selected from our registry. Among them, those with fewer than 10 LNs were excluded, based on the assumption that a competent ALND necessitated the removal of 10 or more LNs as defined in previous studies [16,17,18].
Statistical analyses were conducted using SPSS version 25.0 (IBM Inc., Armonk, NY, USA) and GraphPad Prism, version 9 (GraphPad Software). Differences between groups were assessed using the chi-square test for categorical data and one-way ANOVA for continuous variables, subsequent to confirmation by Levene’s test for equality of variances. The primary outcome was recurrence-free survival (RFS), while overall survival (OS) was analyzed as the secondary outcome. RFS was defined as the interval from breast cancer diagnosis to the initial recurrence, including LRR, distant metastasis, or any cause of death. OS was defined as the duration from breast cancer diagnosis to death from any cause. Kaplan-Meier survival estimations were implemented for RFS and OS, and survival curve group disparities were examined via the log-rank test. Variables associated with RFS and OS were ascertained using a multivariate Cox proportional hazard model, with hazard ratio (HR) and corresponding 95% confidence intervals (CI). The analysis of risk factors for additional metastases in SLNmi patients was performed using a binary logistic regression model. All statistical tests were two-sided, and a p value < 0.05 was considered statistically significant.
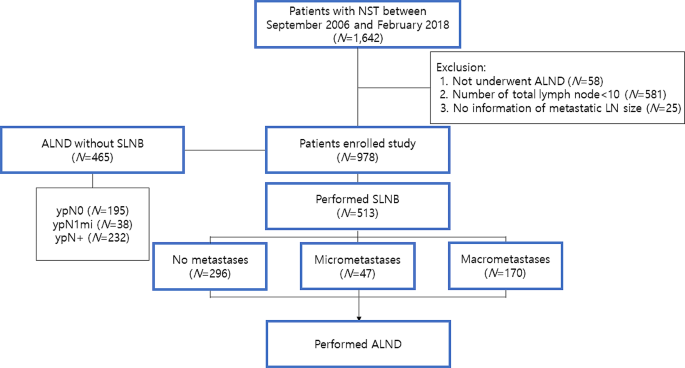
Figure 1 depicts the distribution of axillary surgical procedures among the patients enrolled in our study. Out of the initial 1,642 participants, 664 were excluded due to an inadequate number of axillary LNs or insufficient metastatic LN information. Consequently, 978 patients were analyzed, with a median follow-up duration of 73 months (range, 4-176 months). Among them, 465 (47.5%) patients underwent ALND alone, without SLNB, while 513 (52.5%) patients had SLNB prior to ALND. The clinicopathologic features of the two groups were summarized in eTable 1.
Of the 978 patients examined, 438 (44.8%) exhibited ypN0 after NST, while 89 (9.1%) had ypN1mi and 451 (46.7%) had ypN+. Table 1 summarizes the clinicopathologic characteristics and differences across these three groups. Among the evaluated cohort, 927 (94.8%) patients were cN + pre-chemotherapy. A significant correlation was observed between pathologic tumor size and axillary nodal status. More than half of the patients with ypN0 achieved a breast pathologic complete response (pCR), while this proportion was significantly lower in the ypN + group (7.3%). The rate of breast pCR in patients with ypN1mi was 29.2%, lower than that in the ypN0 group, but higher than in the ypN + group. Moreover, the quantity of dissected LNs was marginally higher in ypN + patients (P = 0.003). The proportion of estrogen receptor (ER)-positive or human epidermal growth factor receptor 2 (HER2)-negative tumors was found to be considerably higher in the ypN1mi and ypN + groups compared to the ypN0 group. The Ki-67 labeling index (LI) was negatively correlated with ypN status. Notably, more patients in the ypN1mi and ypN + groups received adjuvant radiotherapy compared to the ypN0 group.
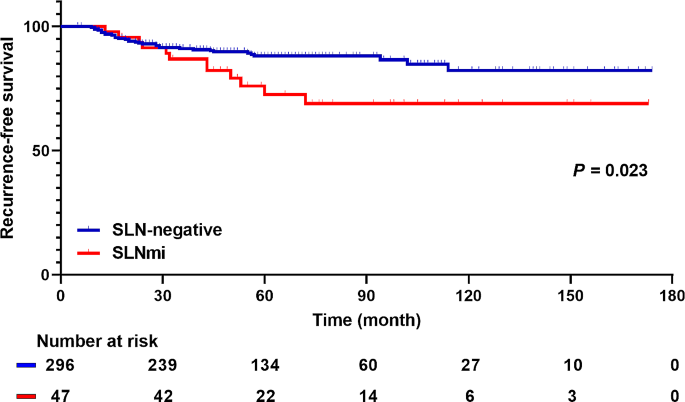
The collective 5-year RFS for all patients was 82%. Broken down by group, the 5year RFS for ypN0, ypN1mi, and ypN + patients were 89%, 87.6%, and 74.1% respectively. Throughout the follow-up period, a total of 183 patients experienced 217 recurrent events. These recurrences manifested as locoregional in 11 patients, systemic in 138 patients, and combined locoregional and systemic in 34 patients. Out of the total patient pool, 85 deaths occurred with a 5-year OS rate of 92.7%. Among the deceased, 70 patients succumbed to breast cancer recurrence, while 15 deaths were attributed to other causes.
Our study showed that patients with ypN0 and ypN1mi had comparable RFS and OS outcomes, while those with ypN + had a negative impact on oncologic outcomes. Notably, axillary LN status could not be accurately ascertained solely by the micrometastases of SLN. Instances of SLNmi often coincided with additional LN metastases and correlated with worse RFS compared to patients who were SLN-negative. Consequently, our findings suggest that axillary staging via ALND in patients with SLNmi should be considered following NST.
The association between residual axillary disease and prognosis is well-documented [19,20,21]. We hypothesized the existence of a subgroup of patients who might exhibit a more favorable prognosis, even in the presence of residual axillary tumor burden, such as micrometastases. Our findings substantiate this, demonstrating that patients with ypN1mi have a more favorable prognosis compared to those with ypN+, and their oncologic outcomes are on par with those of ypN0. Prior to our investigation, only two retrospective studies, to the best of our knowledge, examined residual nodal burden. Nijinatten et al. studied prognosis as a function of metastatic LN size in a single institution [22], in which all patients were cN + and 3.8% of patients were classified as ypNitc/mi. They reported a similar prognosis for ypNitc/mi and ypN0 patients, superior to that of ypN + patients. Our results align with these findings within a similar patient population, despite a higher ypN1mi percentage (9.1%) in our study. Conversely, Wong et al. contended that post-NST patients with isolated tumor cells or micrometastases had a worse prognosis than those with ypN0 in both a single institution cohort and the National Cancer Database (NCDB) [23]. They reported ypN1mi rates of 9.1% and 4.7% in their respective cohorts. However, their study included patients who underwent SLNB without ALND in survival analysis. In contrast, our study exclusively enrolled patients who had 10 or more axillary LNs dissected to optimally evaluate axillary nodal status.
SLNB is a valuable intraoperative tool for predicting axillary LN metastases, though it is observed to yield higher rates of false negatives in NST patients compared to those in a primary surgical setting [24, 25]. The SENTinel NeoAdjuvant (SENTINA) trial demonstrated a FNR of 18.5% when two SLNs were removed, despite clinical conversion to node negativity post-NST [11]. In our cohort, the mean number of removed SLNs was 2.62, resulting in an elevated FNR of 23.8%. Furthermore, we noted that 17.9% of SLN-negative patients had verifiable axillary LN metastases.
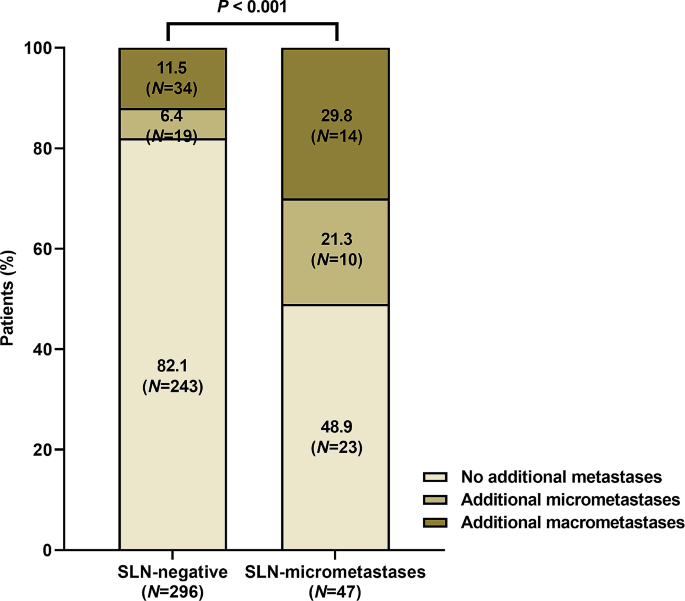
Our findings indicate a substantially higher incidence of additional metastases in patients with SLNmi relative to those with SLN-negative results. Prior to our investigation, Moo et al. documented that 64% of SLNmi patients exhibited non-SLN metastases, a significantly higher figure than the 17% observed in SLN-negative patients [26]. Weiss et al. also reported that 29.4% of cN1 patients with SLNmi had non-SLN metastases, which was not statistically different from patients with SLN-macrometastases [27]. Our study corroborated these findings, revealing additional metastases in 51.1% of SLNmi patients, 58.3% of which were macrometastases. However, in the adjuvant setting, specifically within the American College of Surgeons Oncology Group Z0011 trial, the incidence of additional metastases among SLNmi was considerably lower, at roughly 10% [28]. This discrepancy suggests a heightened likelihood of additional metastases in NST patients with SLNmi compared to those in the adjuvant setting. In a novel discovery, we also found that SLNmi patients exhibited lower RFS rates than SLN-negative patients. Collectively, these findings suggest the necessity of ALND in patients with SLNmi following NST.
In the analysis of risk factors linked to additional metastases in SLNmi patients, a correlation was observed with pathological tumor size exceeding ypT2, ER-positive/HER2-negative subtype, and low Ki-67 LI (≤ 14%). These findings can be contextualized within the sphere of NST responsiveness. It is well established that ER-positive/HER2-negative tumors present a lower overall response rate [29, 30]. Additionally, low levels of Ki-67 LI associated with reduced pCR rates [31, 32]. Consequently, it can be inferred that SLNB accuracy is interrelated with NST response, and SLNmi is more likely to exhibit additional metastases in patients demonstrating a suboptimal response to chemotherapy. In the study by Weiss et al., it was also reported that all SLNmi patients with additional metastases had hormone receptor-positive subtype [27].
One limitation of this study includes the potential bias stemming from its retrospective design and small sample size of SLNmi patients. However, we were able to source relatively uniform and reliable clinicopathological and prognosis data from two institutions and endeavored to accurately evaluate the axillary nodal status. Nonetheless, we were unable to consider the clinical nodal status after NST as determined by imaging modalities. Future studies combining SLNB results with chemotherapy response evaluations via imaging examination in SLNmi cases may be necessary, as some studies suggest that the accuracy of axillary nodal status prediction can be enhanced when imaging examination results are integrated with SLNB outcomes [33]. Another limitation is the inclusion of cN0 patients in our study cohort, which introduces the possibility of bias in the analysis. However, cN0 patients constitute only 5.2% of the entire cohorts, and since there was no statistical difference between the ypN stage groups, we think their impact is likely to be minimal. enrolled patients. In addition, due to the retrospective nature, the authors did not directly participate in the confirmation of micrometastases detection in final pathology. However, the two institutions where the patients were enrolled have a common protocol for detection of LN metastases, and this has been reconfirmed through consultation with experienced breast pathologist.
In conclusion, SLNmi is an adverse prognostic indicator as a critical predictor of additional metastases, while ypN1mi does not significantly impact patient prognosis when compared with ypN0. Especially, in patients with a poor NST response, SLNmi increase the possibility of additional metastases. As such, additional ALND should be considered for verifying axillary nodal status in patients presenting with SLNmi.
No datasets were generated or analysed during the current study.